Introduction
Sarcoidosis is a systemic granulomatous disease of unknown etiology surrounding an inciting antigenic exposure that triggers a dysregulated immune response leading to the formation of non-caseating granulomas; the complex interplay of the innate and adaptive immune responses play a role in this.1 Exposure-related sarcoidosis is not clearly defined, but several studies highlight environmental associations not only with disease development but also with phenotypic expression, severity, and pattern of organ involvement. For example, epidemiologic analysis of World Trade Center (WTC) first responders has shown higher rates of sarcoidosis relative to the civilian population.2 In the military population, sarcoidosis was first described in 1949, with conflicts in the Middle East and Southwest Asia bringing to light the respiratory conditions associated with deployment and exposure to airborne particulate matter such as geological dust, smoke from burn pits, and heavy metal condensates.3
In 2014, the United States Department of Veterans’ Affairs established the Airborne Hazards and Open Burn Pit Registry (AHOBPR), allowing veterans exposed to burn pits to voluntarily enroll and report their current health status.3,4 Data collected through this registry indicated that former service members exposed to burn pits exhibited higher rates of sarcoidosis compared to the general population. Antigen exposure associated with burn pits, including metals, dioxins, polycyclic aromatic hydrocarbons, and particulates may lead to dysregulated immune response implicated in disease pathogenesis.
Here we present a case of a former service member with osseous and bone marrow sarcoidosis and a history of deployment to Afghanistan with burn pit exposure.
Case presentation
A 52-year-old year old white male veteran presented with a four-month history of progressive back pain accompanied by unintentional weight loss of thirty pounds over four months, chills, and anorexia. He also reported worsening of severe lower extremity pain with intermittent numbness on the anterolateral thigh. Review of systems was otherwise negative.
Comorbid conditions include coronary artery disease, diabetes mellitus, hypertension, and sciatica. Home medications included Aspirin (81 mg daily), Atorvastatin (40 mg daily), Gabapentin (100 mg three times a day), Hydralazine (10 mg twice daily), Hydrochlorothiazide (50 mg daily), Jardiance (25 mg daily), Lantus (20 units daily), Metformin (500 mg twice daily), Oxycodone (10 mg every 6 hours as needed), and tizanidine (4mg three times a day). He had no relevant family history. He had an eight-pack year smoking history and reported miliary service with deployment to Afghanistan. The patient reported environmental exposures involving burn pits and aircraft exhaust fumes approximately twenty years prior to symptom onset.
Physical exam included normal vital signs, with normal cardiac and respiratory system exams. There was left testicular tenderness with several palpable lymph nodes in the neck and pelvic area. Neurological exam revealed normal strength, sensation, and reflexes of the upper and lower limbs. Laboratory studies were normal (WBC 8.4 k/mm3, HgB 14.8 g/dL, platelets 323 K/mm3, calcium 9.8 mg/dL, vitamin D, 25-Hydroxy 31.70 ng/ml). Baseline electrocardiogram demonstrated normal sinus rhythm.
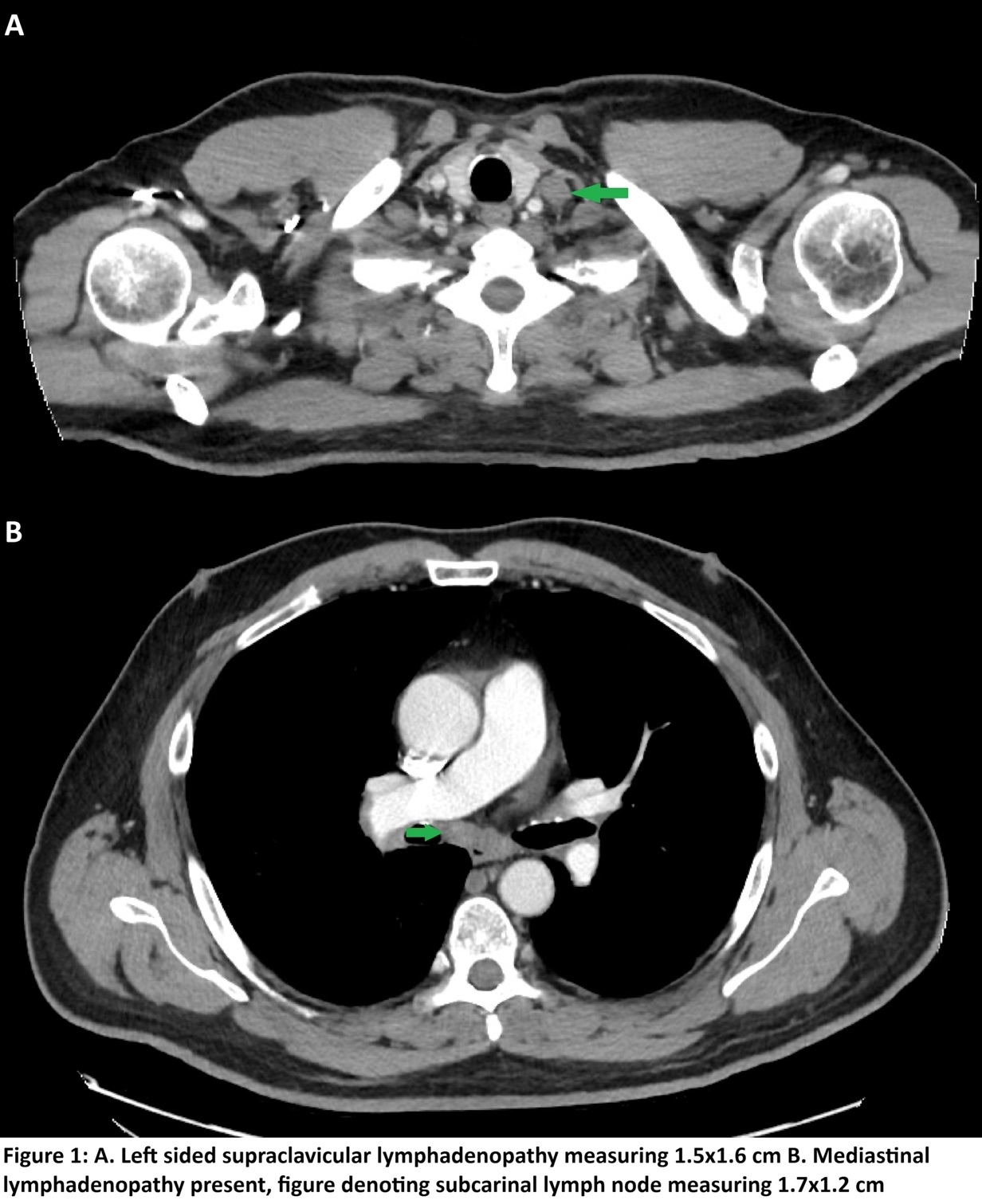
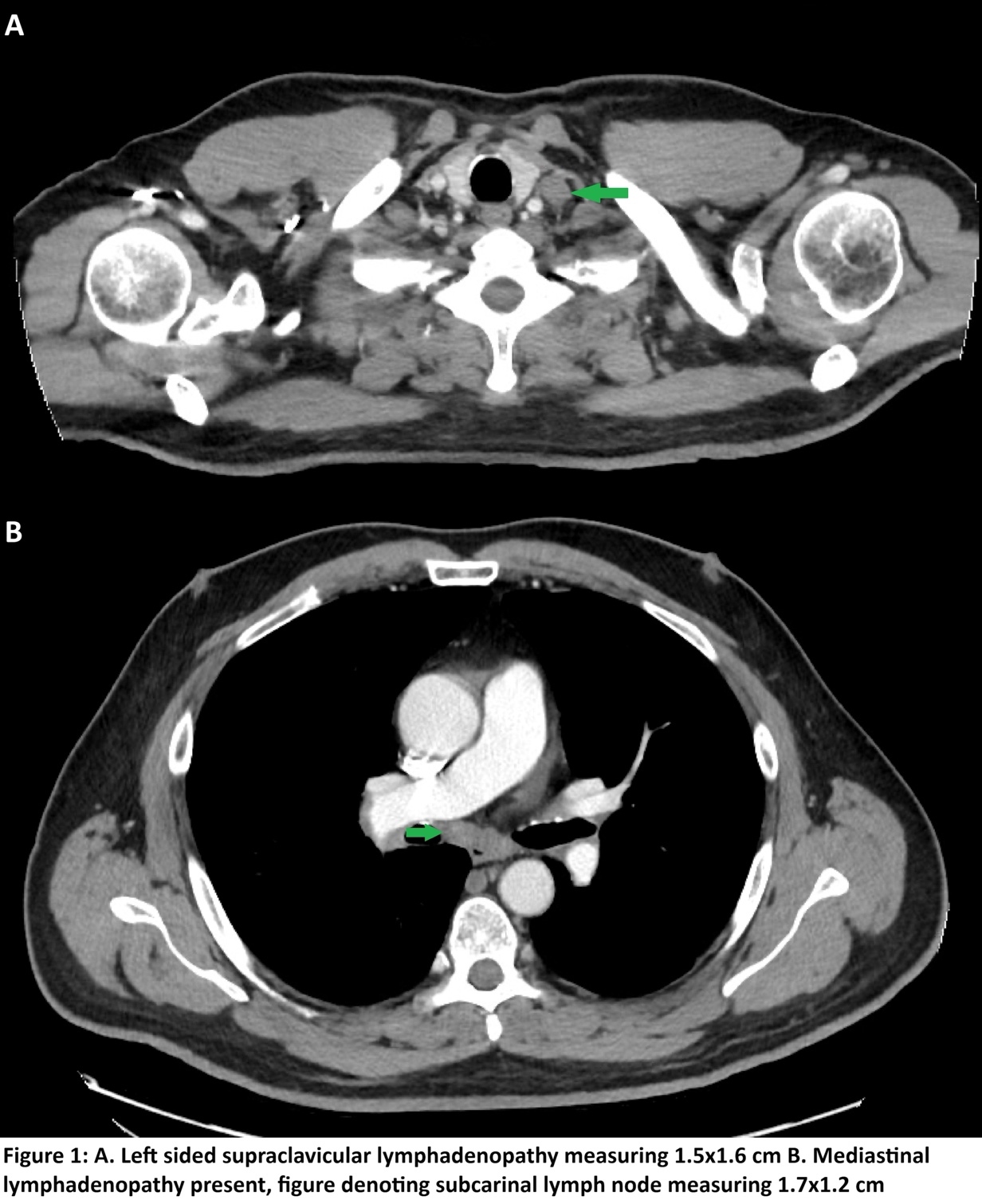
Magnetic resonance imaging (MRI) of the spine was ordered for worsening symptoms, revealing multifocal T1/T2 hypointense marrow lesions of the spine concerning for metastatic disease. The patient was subsequently referred to orthopedics for further evaluation. A comprehensive workup was initiated, including computed tomography (CT) of the chest, abdomen, and pelvis, as well as a bone scintigraphy scan. The bone scan was unremarkable; however, CT imaging demonstrated multistation lymphadenopathy involving the supraclavicular, mediastinal, bilateral hilar, and retroperitoneal lymph nodes.
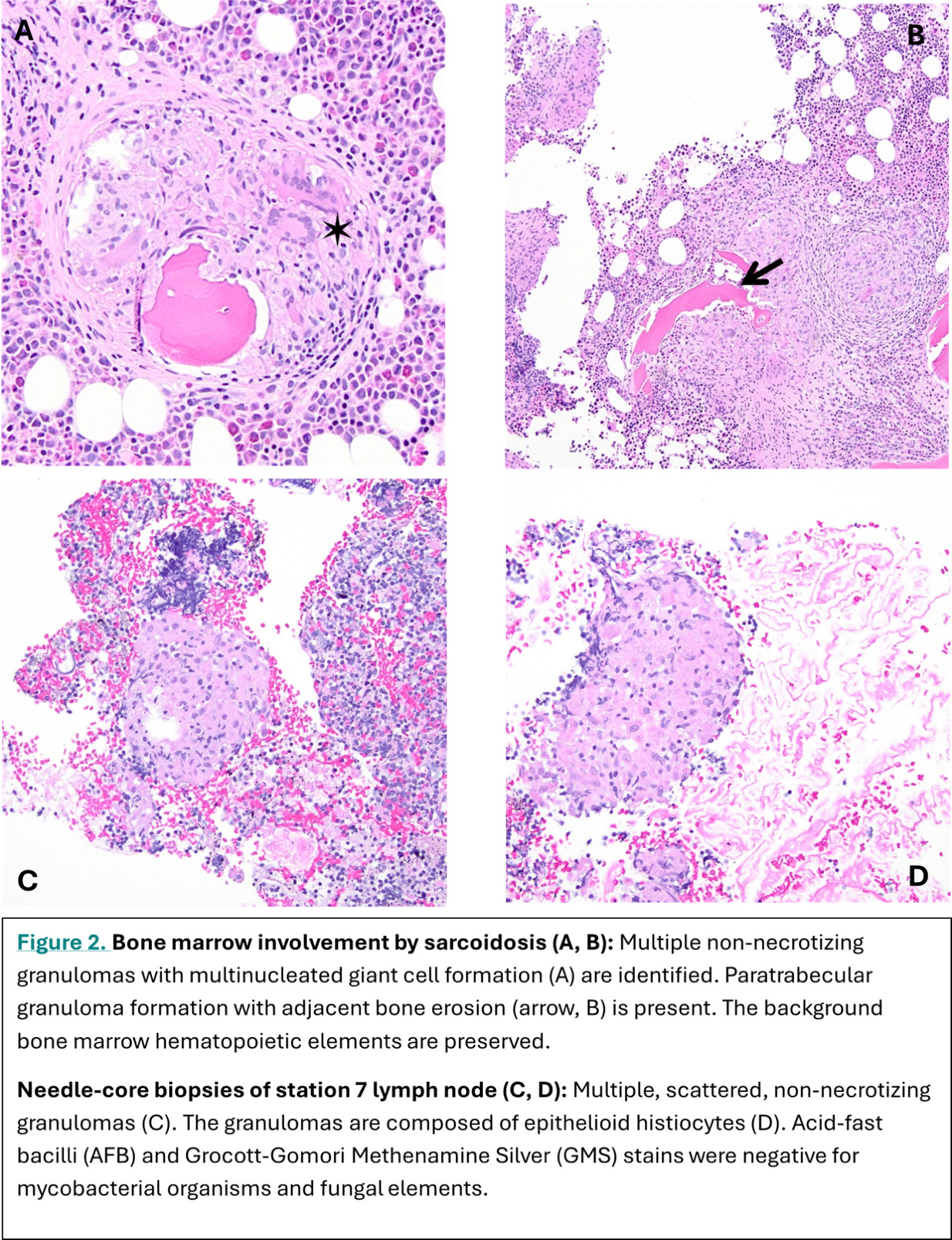
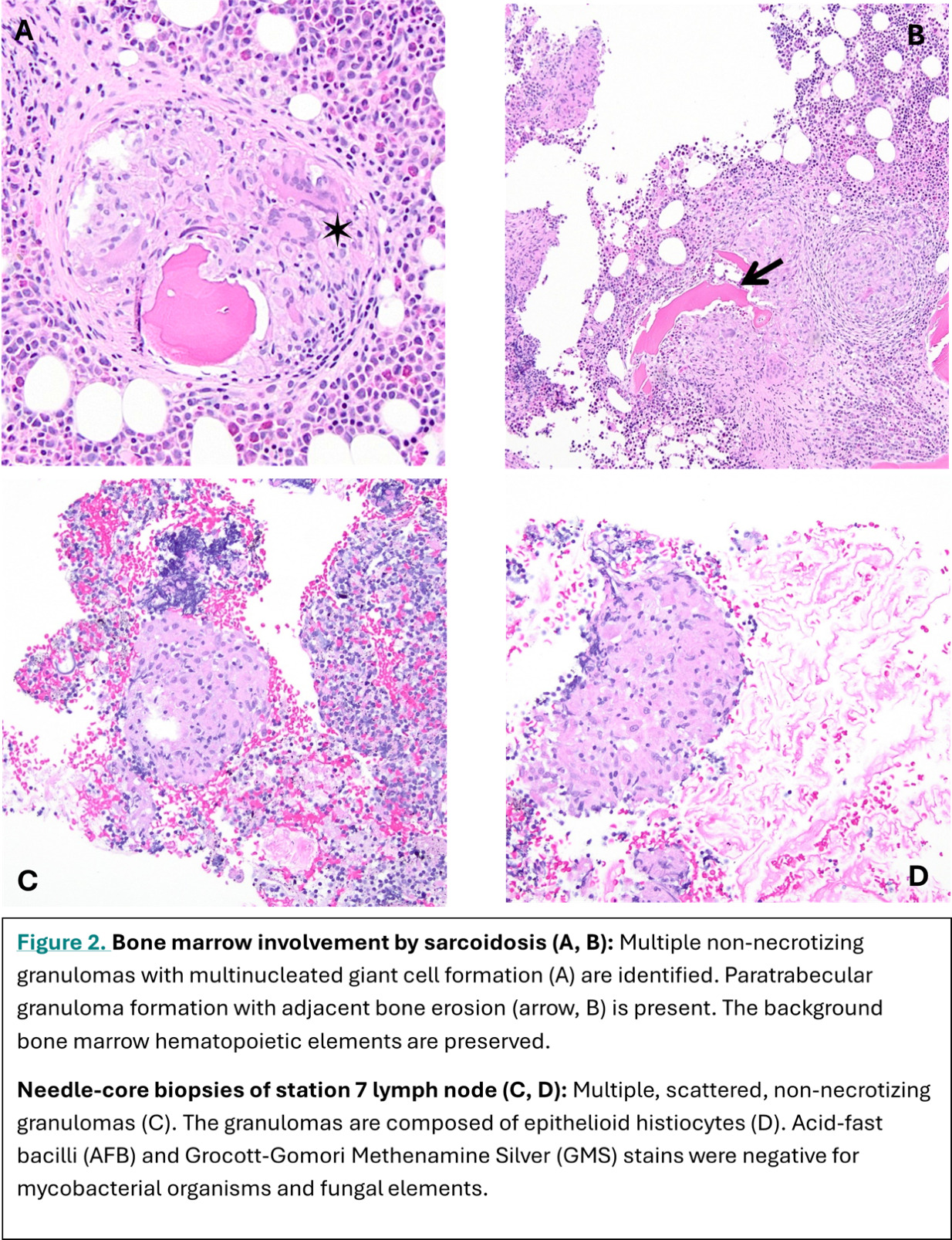
Given the constellation of symptoms and diffuse lymphadenopathy, lymphoma was initially suspected. The patient underwent a bone marrow biopsy and was referred to interventional pulmonology for endobronchial ultrasound (EBUS) guided transbronchial biopsies of hilar lymphadenopathy. Lymph node stations 7, 11L, and 11R were ultimately biopsied. Bone marrow pathology revealed preserved trilineage hematopoiesis with multiple non-necrotizing granulomas, including a paratrabecular granuloma with adjacent bone erosion (Figure 1A & 1B). EBUS samples from station 7 demonstrated multiple, scattered, non-necrotizing granulomas composed of epithelioid histiocytes (Figure 1C & 1D). All biopsies obtained were sent for routine cytology, microbiology, and flow cytometry to further exclude other sources for the granulomas. He was referred to the sarcoidosis clinic, and a multidisciplinary discussion confirmed a diagnosis of sarcoidosis with bone marrow involvement.
Due to significant symptoms, steroid therapy (Prednisone with an initial dose of 40 mg tapered to 20mg daily) was initiated, followed by the addition of Methotrexate, titrated to 15mg weekly, with plans to increase as tolerated. Due to significant hyperglycemia, prednisone has been tapered at a quicker rate than previously planned. The patient was promptly referred for a retinal exam, pulmonary function testing, and routine laboratory testing to assess for other organ involvement. PET-CT obtained upon presentation to the sarcoidosis clinic demonstrated decreased hypermetabolic activity in thoracic lymphadenopathy but ongoing persistence of areas of hypermetabolism within the bone marrow, as well as a scattered focal site of FDG uptake at T1 vertebral body. Despite a negative bone scintigraphy scan, the hypermetabolic findings above both further support the diagnosis of osseous and bone marrow sarcoidosis and signify ongoing sarcoidosis activity. The patient has been tolerating medications well, but unfortunately continues to have ongoing bone pain in the lower extremities. The patient remains under close follow-up, with ongoing titrations of dual immunosuppressive therapy and periodic PET-CT imaging to monitor disease activity.
Discussion
Sarcoidosis is a global disease with prevalence varying by geographic region, sex, and ethnicity. Most epidemiologic data are derived from large healthcare databases. With an estimated incidence of 8 to 11 per 100,000 per year in the general population, the incidence varies by race and ethnicity, and is 3 per 100,000 among Asian individuals, 4 per 100,000 among Hispanic individuals, 8 per 100,000 among White individuals, and 18 per 100,000 among black individuals. The reported prevalence of sarcoidosis in the United States is approximately 50-60 per 100,000 persons, with regional variation, including higher prevalence in the Northeast compared to the Western United States.1 Among U.S. Veterans, prevalence estimates are consistently higher, increasing from approximately 79 per 100,000 to 141 per 100,000.3,5
Much of what is known about sarcoidosis among U.S. Veterans comes from case series among subspecialty clinics, metabolomic studies comparing civilian and veteran populations, and established cohorts, including the Millennium Cohort Study and the Airborne Hazards and Open Burn Pit Registry (AHOBPR).4,6 The incidence and prevalence of sarcoidosis are clearly higher among Veterans than non-veterans, as it has been associated with their occupational and environmental exposures related to deployment, such as burn pits. These pits are known to produce dense plumes of smoke containing particulate matter, toxic gases, and carcinogenic compounds.3 This exposure is postulated to drive a distinct molecular phenotype of disease due to very distinct plasma metabolic or metallomic profiles.7 The disease can be diagnosed many years after deployments, which creates another layer of difficulty when studying these associations.
Bone marrow involvement is approximated to occur in 10-17% of cases, though rates may be higher but underrecognized.8–10 Diagnosing bone marrow sarcoidosis can be challenging, as a biopsy is required for confirmation. Patients may present with cytopenias, such as anemia, thrombocytopenia, or leukopenia, or a complete absence of symptoms.9 In individuals with osseous sarcoidosis, patients may have severe, debilitating bone pain as a symptom. Imaging may reveal lytic or “moth-eaten” lesions, because of its radiographic resemblance to metastatic malignancy on PET/CT will cause the leading diagnosis to be malignancy.11 Management of osseous and bone marrow sarcoidosis, given its rarity, is largely guided by anecdotal evidence and treatment responses observed in other extrapulmonary manifestations.8,9
Accumulating observational data suggest a link between military-related exposures and increased risk of sarcoidosis and extrapulmonary manifestations. We attempt to establish such an association in our case and highlight the need for further rigorous epidemiological and mechanistic studies to establish a causal relationship between environmental exposures and sarcoidosis, particularly among our veteran population. The goal is to inform mitigation and prevention efforts, as well as screening and diagnosis of such complex diseases.