Introduction
Esophago-pericardial fistula (EPF) is a rare condition in which a connection forms between the esophagus and pericardium, allowing gas, gastric debris, and microorganisms to pass into the pericardial space. Based on data acquired since 2000, this entity will be most frequently encountered clinically following an ablation for atrial fibrillation.1 Malignancy, esophageal surgery, foreign body or caustic ingestion, and trauma are additional described etiologies.1–3 However, EPF is also an unusual complication of Boerhaave syndrome.4 Boerhaave syndrome describes transmural esophageal perforation from increased intraluminal pressure against a closed cricopharyngeus, classically secondary to repeated emesis. Presenting signs and symptoms are nonspecific, so imaging can play a crucial role in early detection. A CT chest/abdomen with oral contrast (“CT esophagram”) was essential to clinching the diagnosis in our case. Early detection of EPF and directed management are paramount for improving patient outcomes.4,5 In addition to broad-spectrum antibiotics and withholding oral intake, source control with either surgery or endoscopy is imperative.4 Endoluminal vacuum therapy, in which polyurethane sponges are inserted endoscopically into the cavity as a vacuum is applied externally, is a less invasive method that can be used for treatment, as it was for our patient.6
Case Report
A 36-year-old male with a history of polysubstance use presented to the emergency department with epigastric abdominal pain and recurrent emesis. Vitals were evident of acute decompensation, with temperature 37.4ºC, HR 132 bpm, BP 87/60 mmHg, and oxygen saturation 100% 2L nasal cannula. Physical exam noted weak pulses in all extremities.
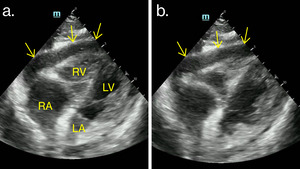
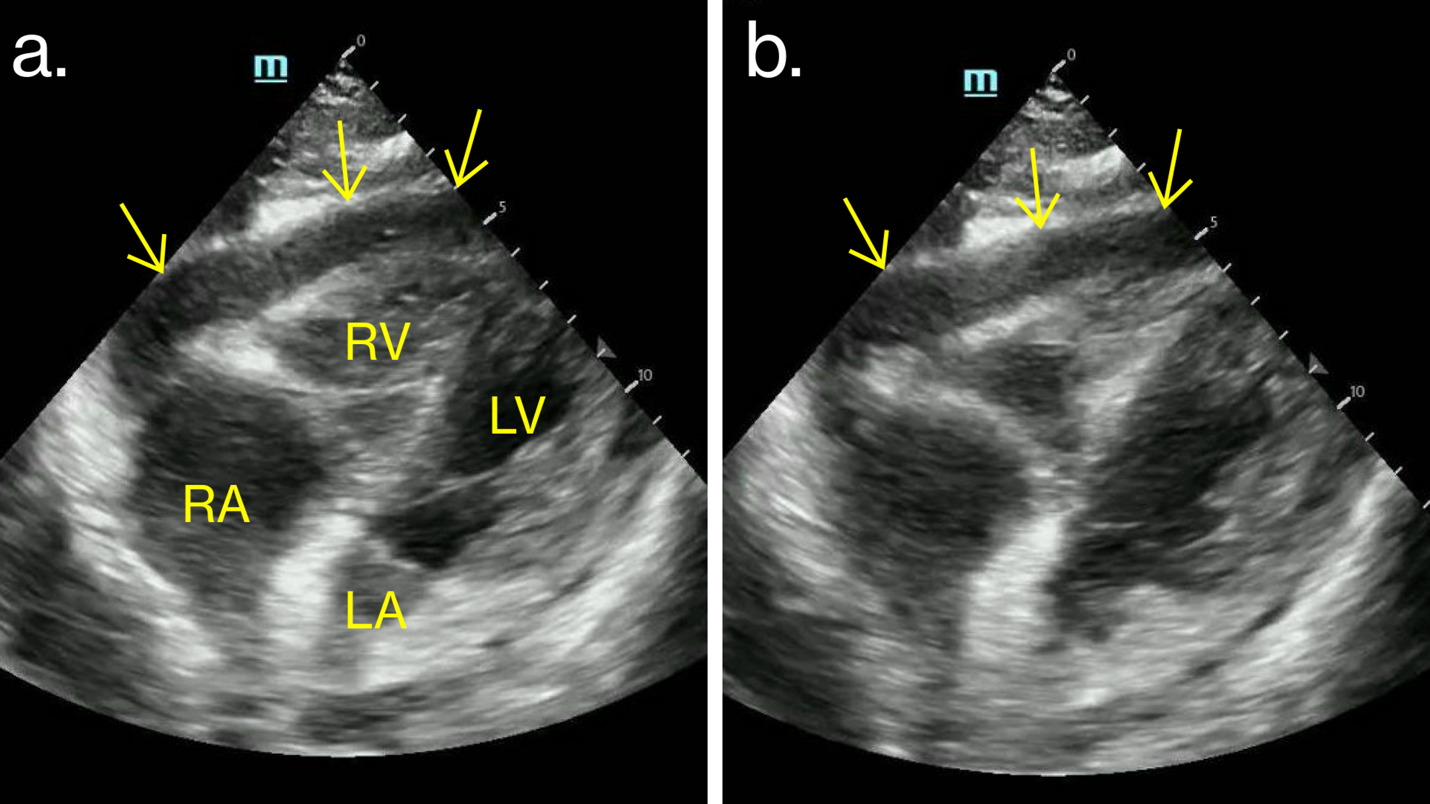
He was started on norepinephrine for blood pressure support, but became lethargic. EKG demonstrated ST elevations throughout the inferolateral leads, concerning for acute infarct versus pericarditis. Cardiac point-of-care ultrasound (POCUS) showed a large pericardial effusion (Fig. 1). Blood pressure measured by femoral arterial line exhibited pulsus paradoxus, confirming tamponade physiology. The patient suddenly went into cardiac arrest and was intubated. An emergent pericardiocentesis was performed, yielding 20 mL of brown fluid mixed with air. Return of spontaneous circulation was subsequently achieved.
Given the pericardiocentesis findings, a CT esophagram was performed to evaluate for EPF. Per institutional protocol, this consists of a CT chest/abdomen with venous phase intravenous contrast, plus oral contrast. In this case, Omnipaque-350® was administered via orogastric tube.
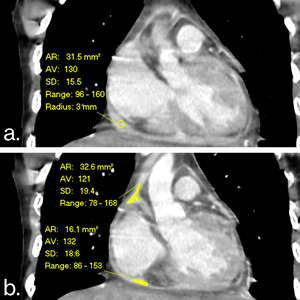
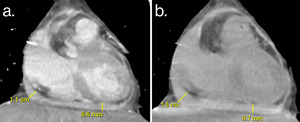
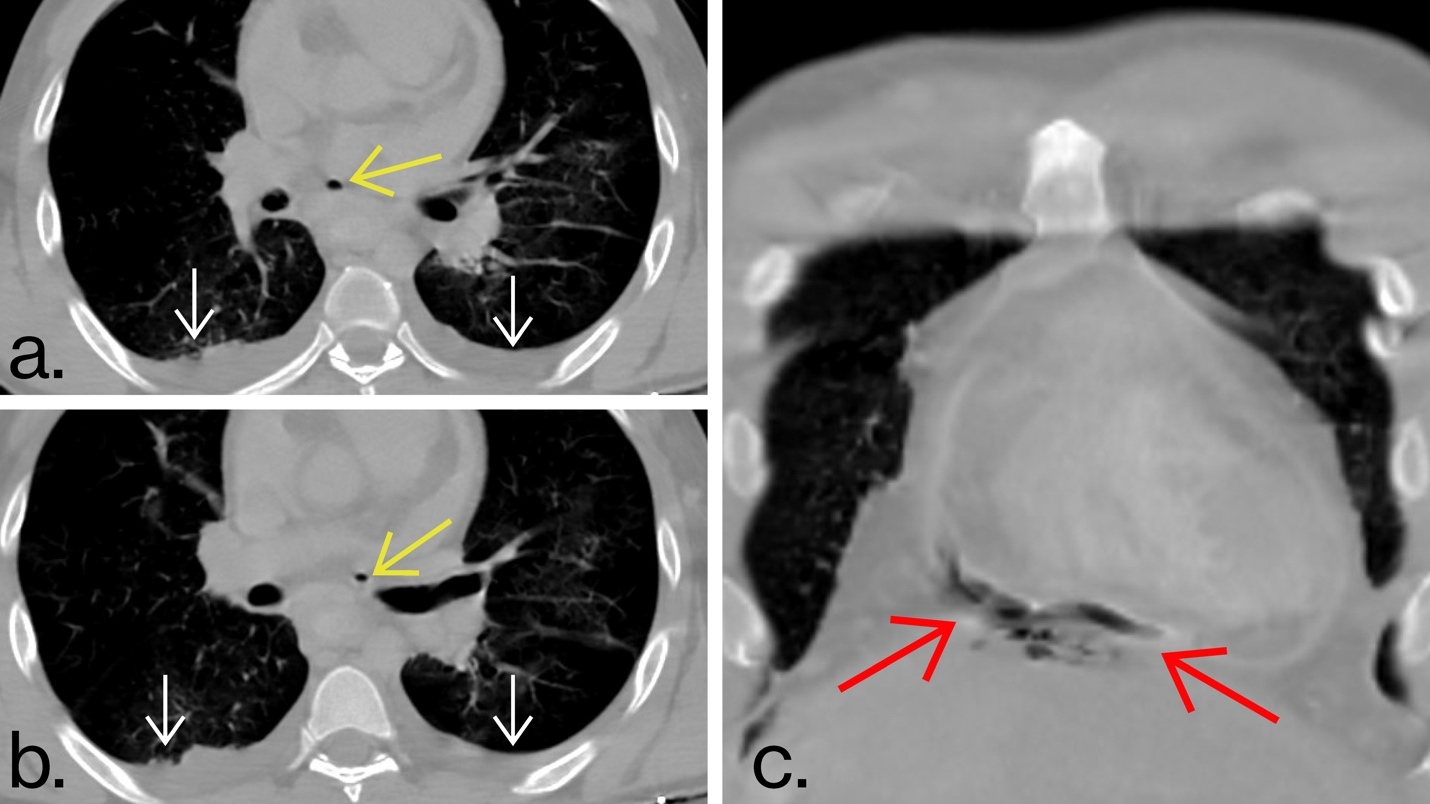
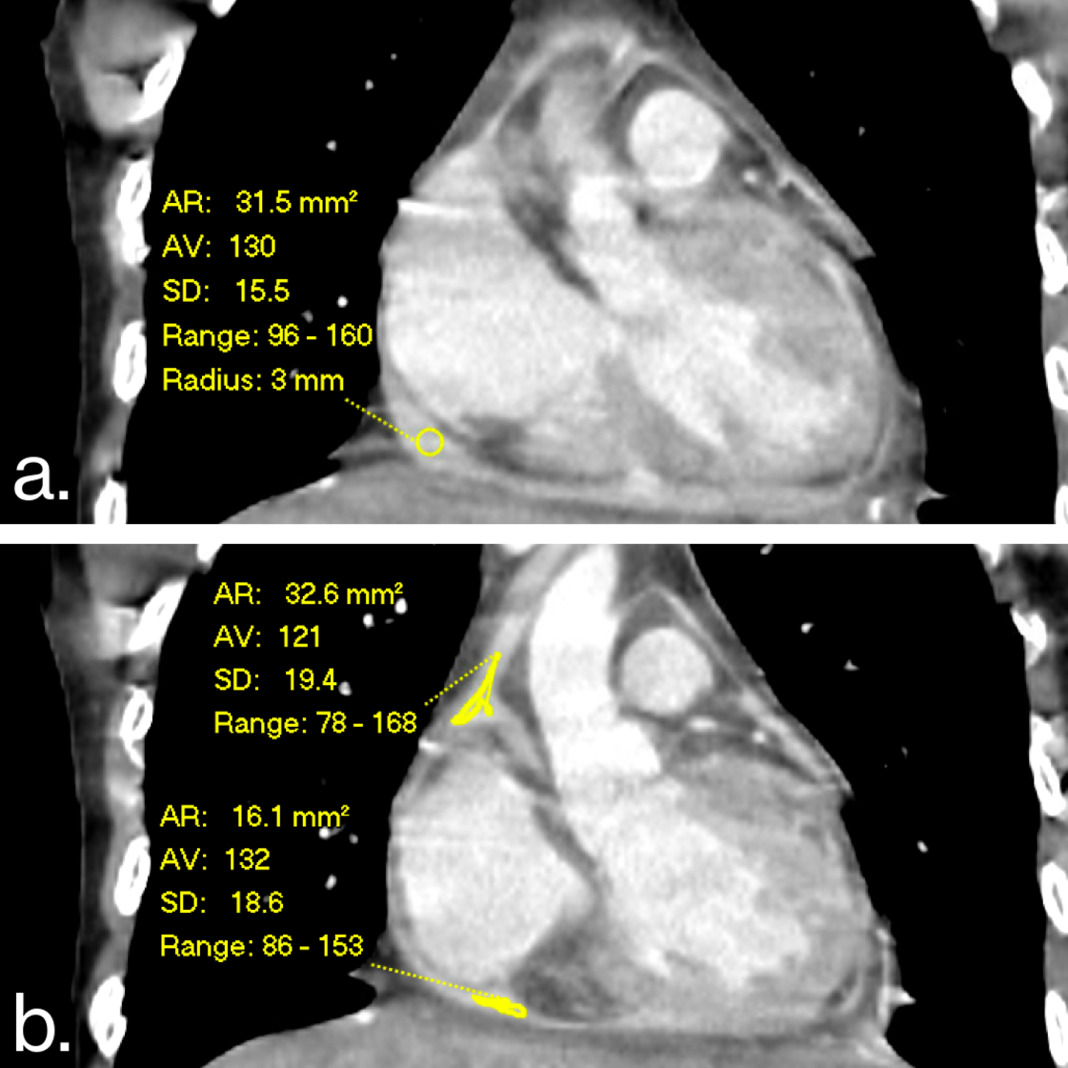
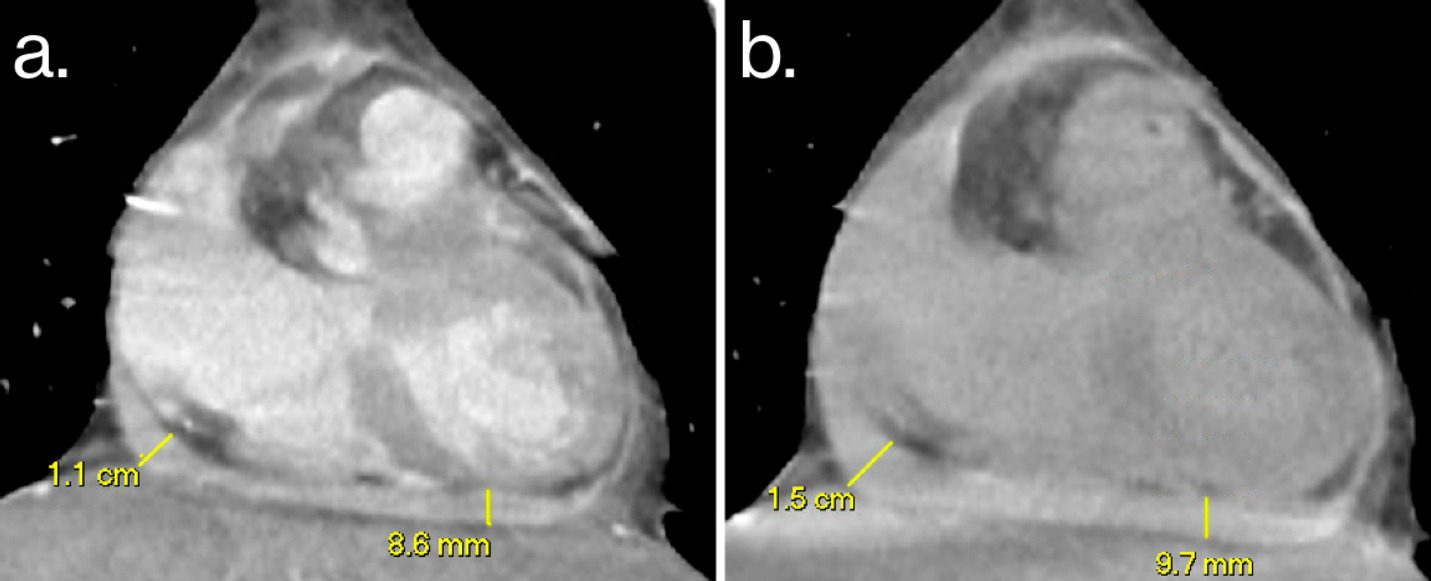
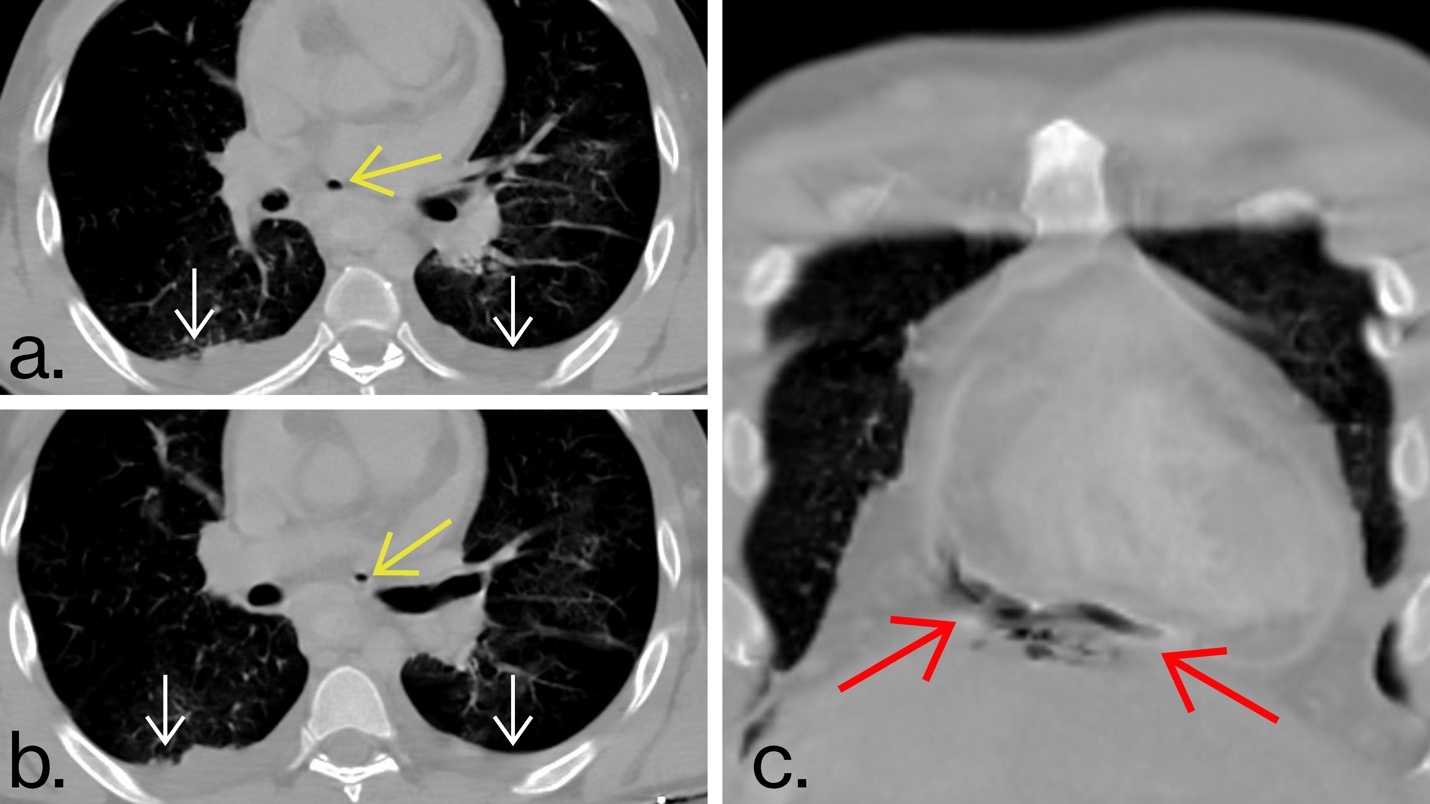
CT esophagram demonstrated a large amount of hyperattenuating pericardial fluid, measuring 121-132 HU, far greater than the expected normal values between 0-10 HU. This confirmed that there was oral contrast mixing into the pericardial space (Fig. 2). These initial images also showed suboptimal distension of the esophagus, with the tip of the orogastric tube positioned within the distal esophagus. In an attempt to directly visualize the fistula, the orogastric tube was retracted into the upper esophagus, oral contrast was re-administered, and the scan was repeated. The two CTs were performed six minutes apart, with a combined total of 100 mL of oral contrast. Following the second bolus of oral contrast, the hyperattenuating pericardial effusion had enlarged, though the fistula was still not apparent (Fig. 3). Both pneumomediastinum and pneumopericardium were present (Fig. 4). Pneumopericardium could have been attributed to the recent pericardiocentesis and/or EPF. However, the presence of multiple foci of gas in the middle and posterior mediastinum elevated suspicion for an esophageal rupture in the setting of Boerhaave syndrome. Also noted were small bilateral pleural effusions.
These imaging findings confirmed the diagnosis of EPF, which was likely secondary to Boerhaave syndrome, given the history of prolonged, forceful emesis. The patient was emergently taken to the surgical suite for washout, pericardiotomy with drain placement, and upper endoscopy. Per the operative report, gastric contents were drained from the pericardium upon creation of a pericardial window. Esophageal ulceration and perforation were seen superior to the esophago-gastric junction and treated with endoscopic vacuum-assisted closure. A percutaneous gastrostomy was created to bypass the perforation.
Cultures from the pericardial fluid produced polymicrobial organisms consistent with gastrointestinal flora. Intra-operative pathology specimens resulted as ulcerated esophageal mucosa without malignancy. Unfortunately, the remainder of the patient’s hospital course was marked by complications, including pericardial abscess, empyema, pulmonary emboli, Enterococcus bacteremia, septic shock, acute renal failure, and diffuse alveolar damage, ultimately resulting in tracheostomy and ventilator dependence. Four weeks after presenting, the patient was transitioned to comfort care, after which he passed away.
Discussion
EPF is a grave condition conferring a poor prognosis that is commonly caused by malignancy, surgical intervention, or caustic injury.2 Our case exemplifies an unusual nonsurgical presentation resulting from esophageal rupture in the setting of Boerhaave syndrome.
Early detection and treatment of EPF are of the utmost importance, as mortality can approach 90% when untreated, and even in a recent meta-analysis of cases since 2000, the reported mortality rate was alarmingly high, at 32.6%.1,6,7 Unfortunately, vague presenting symptoms such as emesis, epigastric/chest pain, fever, dysphagia, and dyspnea can pose diagnostic ambiguity.3,7,8 As in this case, multi-lead ST elevations on EKG could raise clinical suspicion for pericarditis.2 Yet understanding the key imaging findings highlighted in this case significantly contributes to reaching a timely, accurate diagnosis.
Cardiac POCUS and transthoracic echocardiogram are limited in clinching the specific diagnosis of EPF, but can confirm the presence of a pericardial effusion, possibly with internal debris.1 Findings of cardiac tamponade may be present, although this ultimately depends on the volume of pericardial fluid and its rate of accumulation.8
CT esophagram can offer distinct advantages over fluoroscopy as the first-line imaging modality for suspected Boerhaave syndrome and EPF. In a recent literature review, CT esophagram demonstrated superior sensitivity for detecting esophageal perforation, approaching 100%, while single-contrast fluoroscopic esophagram had a lower sensitivity of 70-90%.9 Additionally, CT esophagram is more readily available, provides anatomic context, and evaluates for alternative diagnoses. Endoscopy as an initial diagnostic tool remains controversial due to concerns for worsening propagation of existing esophageal tears.4 The primary imaging findings of EPF on a CT esophagram include: hyperattenuating pericardial fluid, pericardial effusion, pneumopericardium, and/or pneumomediastinum. It is paramount to note that, as in our case, nonvisualization of the fistula does not exclude the diagnosis. Raising early suspicion and inter-disciplinary collaboration between clinicians and radiologists are both essential for expeditious management, in turn conferring the greatest chance of survival.