Introduction
Cosmetic procedures, including gluteal augmentation, are increasingly popular. Gluteal augmentation, also referred to as the “Brazilian butt lift,” was among the top five cosmetic surgical procedures in the United States in 2023, according to the American Society of Plastic Surgeons’ Procedural Statistics Report.1 Augmentation procedures are used to reshape the buttocks, thighs, or hips, and are often accomplished through silicone implants or fat grafting. The FDA currently does not recommend using soft tissue fillers for breast or buttocks augmentation; however, reports of off-label fillers have recently increased, with disfiguring and devastating outcomes.2–5
Large volume subcutaneous injection of permanent fillers, such as silicone, is associated with a number of complications, including granulomas, tissue necrosis, embolization, and even multi-organ damage.4,6 Large-volume injections performed in non-medical environments pose additional risks, such as non-medical staff administering non-medical-grade products using non-sterile equipment. In addition to silicone, large volume injection of castor oil has been previously described, leading to multi-organ failure within 24 hours following the procedure.5
We report a case of cosmetic gluteal injection of castor oil causing severe hemolysis, multi-organ failure, and death. The University Institutional Review Board reviewed this work and determined it did not constitute human research and was exempt from informed consent.
Case Presentation
A 26-year-old woman presented to the emergency department as a transfer from Mexico following bilateral hip and buttock injections for gluteal augmentation. Few details of the procedure are known, but according to her family, she was found unresponsive at her home in Mexico shortly after undergoing a “cosmetic procedure” performed in a residential home near the US-Mexico border.
During air transport, the patient had multiple seizures and was subsequently intubated. On arrival, the patient was comatose with a Glasgow Coma Scale of 3T. Her physical exam revealed bilateral fixed and dilated pupils, epistaxis from her oropharynx and nares, tachycardia, and hypotension requiring high-dose vasopressors. The patient’s bilateral hips and buttocks had visible needle puncture sites and pen markings, indicating injection sites. These areas also exhibited significant edema, erythema, and ecchymoses, consistent with tissue inflammation and hemorrhage due to injections.
Initial labs revealed anemia with a hemoglobin 5.2 g/dL (52g/L), severe hemolysis with coagulopathy due to disseminated intravascular coagulation (DIC), with a total bilirubin = 2.7 mg/dL (normal range = 0.2–1.3 mg/dL), indirect bilirubin = 1.5 mg/dL (normal range = 0.2–1.0 mg/dL), direct bilirubin = 1.2 mg/dL (normal range <0.3 mg/dL), D-dimer >7.65 microg/mL, INR = 2.6, platelets = 135,000/microL (normal = 130,000–450,000/microL, and a few schistocytes. An initial ABG showed a pH of 7.04, indicating severe metabolic acidosis with a lactate of 13.6 mmol/L. Her triglycerides were also markedly elevated at 5472 mg/dL (normal < 150 mg/dL). The remainder of her laboratory tests were unobtainable because the lab reported her severe hemolysis interfered with all colorimetric assays.
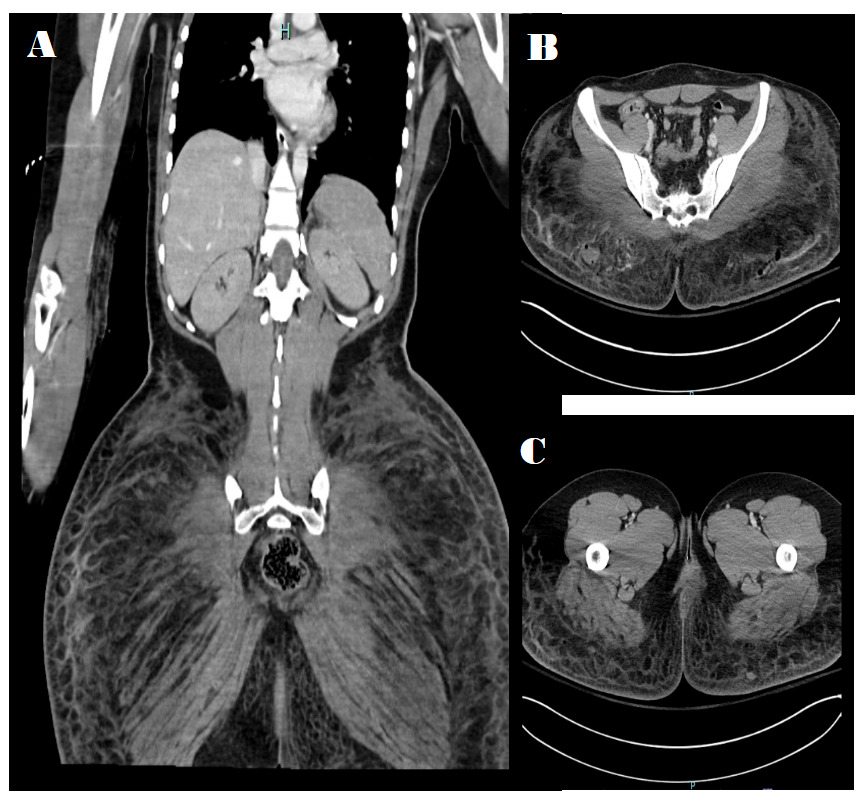
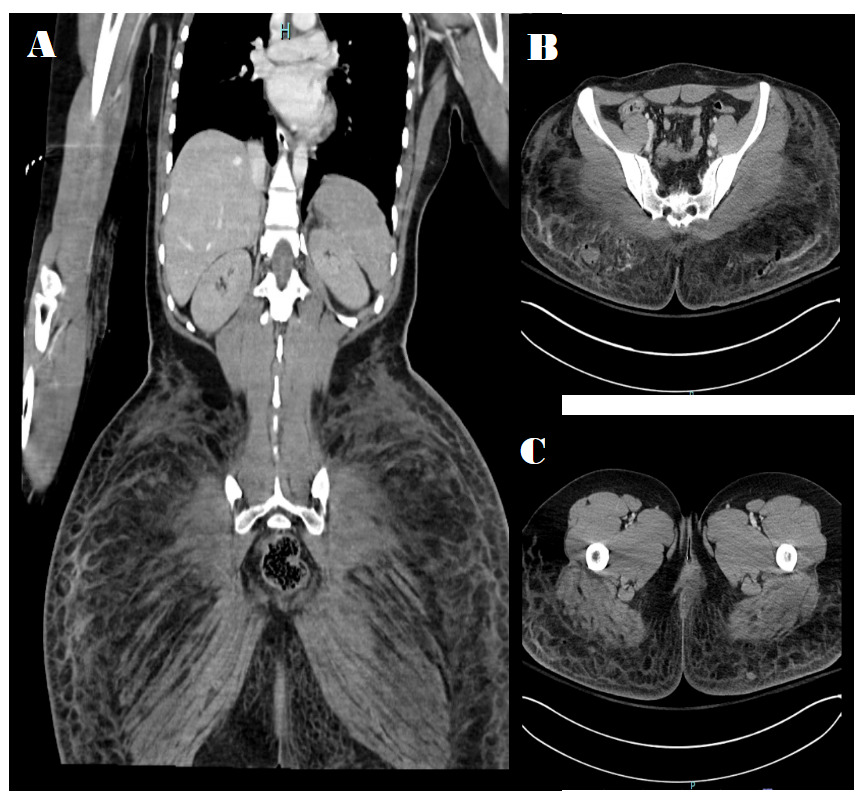
Initial CT of the head revealed bilateral subdural hematomas, measuring 6 mm on the right and 4 mm on the left, as well as small scattered subarachnoid hemorrhages. CT of the pelvis revealed diffuse fat stranding and subcutaneous infiltration of the gluteal region (density 10-20 HU) with punctate foci of gas consistent with subcutaneous injection (Figure 1).
The patient was admitted to the ICU for further management and treated for shock with high-dose vasopressors and broad-spectrum antibiotics (vancomycin, piperacillin-tazobactam, and clindamycin), her anemia was treated with leukoreduced red blood cells (RBCs), and her coagulopathy was corrected with transfusions of FFP and cryoprecipitate. By the second day of her hospital course, her lactic acidosis and coagulopathy had significantly improved, but the hemolysis persisted. Castor oil injection was suspected based on a previously published report of castor oil injections causing severe hemolysis.5 She was treated with one session of plasmapheresis based on the suspicion that her elevated triglycerides represented intravascular castor oil. However, triglyceride levels immediately after plasmapheresis were unchanged, suggesting severe hemolysis interfering with the triglyceride measurement was a more likely explanation. Her triglyceride levels trended down as her hemolysis improved. Cultures of blood and urine showed no growth of bacteria. Tissue cultures taken from the buttock revealed no growth of aerobic or anaerobic bacteria and were negative for acid-fast bacilli (AFB). Bronchoalveolar lavage samples were negative for respiratory pathogens.
A sample of urine that had been obtained shortly after arrival was sent for ricinine testing to the Arizona Department of Health Services’ Bureau of State Laboratory Services, which is part of the United States Laboratory Response Network (LRN) (https://www.cdc.gov/laboratory-response-network/php/about/index.html). Ricinine, a biomarker for castor oil, was confirmed in the patient’s urine via quantitative High-Performance Liquid Chromatography (HPLC/MS-MS); however, it was below the linear threshold of the assay to allow exact quantification.
Unfortunately, while the patient clinically stabilized, it became clear that her neurologic injury was quite severe, meeting criteria for brain death. Her family chose organ donation, and her liver, lungs, and heart were successfully transplanted.
Discussion
As the popularity of hip and buttock augmentation rises, large-volume injections of unapproved substances are of increasing concern for patients and those who care for them. This case highlights the risks and severe complications of using non-approved substances, such as castor oil, for cosmetic enhancement.
Castor oil, derived from the plant Ricinus communis (aka castor plant), is an oil that has been U.S. Food & Drug Administration-approved for use as a stimulative laxative to treat constipation.7,8 However, other unapproved uses of castor oil have been reported, including orally as an anti-inflammatory, antioxidant, anti-bacterial, and as an eye emollient to treat dry eyes.9 The castor seed contains 40% oil and injected castor oil contains toxic constituents.
Ricin, a protein derived from the castor plant, is a potent toxin and could be used as a bioterrorism weapon or warfare agent.10 Ricin is a ribosome-inactivating protein (RIP) that inhibits ribosome elongation factor binding, preventing protein synthesis, and leading to cell death in tissues throughout the body.11 Ricin has a large, glycosylated protein structure, making it difficult to detect in clinical samples.8,12–14 However, ricinine, an alkaloid also derived from the castor plant, is more readily detectable in clinical samples.15 Some public health labs that are part of the LRN can test for ricinine when evaluating possible exposures to Ricinus communis products.12,16–18
Ricinoleic acid, another bioactive constituent of castor oil, is a primary fatty acid implicated in toxic effects following inappropriate injection.19,20 The surfactant properties of ricinoleic acid lower the surface tension of cellular membranes, promoting the rupture of red blood cells and the release of hemoglobin into circulation.21
Clinical manifestations of injected castor oil toxicity include severe hemolysis and shock, leading to multiple organ failure, followed by rapid deterioration of hemodynamic function and death.22 To our knowledge, there has been only one other report of large volume castor oil injection for cosmetic augmentation leading to severe hemolysis and multisystem organ failure.5
There are many causes of hemolysis, but our patient had no other explanation for her acute clinical presentation. Her mother reported no history of any known drug or medication use that has been associated with hemolytic anemia. Limitations of our case report include that we did not perform urine drug testing using thin-layer chromatography (TLC) and Gas Chromatography-Mass Spectrometry (GC-MS) to assess for all potential medication and drug use, and we did not test for warm or cold agglutinins or G6PD deficiency.
This case provides an opportunity to increase clinicians’ awareness of castor oil and ricin toxicity. Treatment is supportive care as there is no specific antidote. Ricinine testing of clinical samples is used to confirm exposure to castor oil or ricin. Testing may be limited by a lack of local or regional laboratory capabilities, but can be obtained by working with public health departments associated with the LRN. Clinicians with cases of castor oil or ricin poisoning are encouraged to consult their regional poison control center (1-800-222-1222) for guidance on management and to promptly report potential cases to their local, county, and/or state health departments.
This case highlights the critical need for enhanced regulation and education regarding procedures involving unregulated injectable substances. The FDA currently approves only injectable fillers for augmentation of the lips, cheeks, chin, and the dorsal aspect of the hand.23 Injectable skin fillers for body contouring, such as increased breast size or increasing the size of the buttocks, are currently not approved.23 Castor oil is not an FDA-approved or studied filler. Clinicians should consider castor oil toxicity in cases of severe hemolysis following “cosmetic” injections, particularly those performed in non-medical facilities.