Introduction
Sleep plays a critical role in physical health, cognitive function, and emotional well-being. The sleep cycle comprises multiple stages: light sleep, deep (slow wave) sleep, and rapid eye movement (REM) sleep. Each stage serves distinct functions, such as memory consolidation, emotional regulation, and tissue repair. Slow wave sleep (SWS), in particular, is associated with restorative processes, such as growth hormone secretion and immune system strengthening. In contrast, REM sleep is crucial for emotional well-being and cognitive functions like learning and memory processing.1,2 Disturbances in sleep patterns, including reductions in total sleep time (TST), SWS, or REM sleep, are linked to numerous health issues, including cognitive impairments, cardiovascular disease, and mental health disorders.3
Recent literature highlights the importance of the glymphatic system in clearing metabolic waste products, including amyloid-beta and tau proteins, from the brain during SWS, thereby reducing the risk of dementia. Enhanced interstitial fluid flow during SWS promotes the removal of neurotoxic substances, which may protect against neurodegenerative diseases such as Alzheimer’s.4 This process underscores the importance of SWS for long-term cognitive health.
Pharmacotherapy aimed at improving sleep quality and quantity has gained substantial attention as a potential treatment for various sleep disorders, including insomnia and circadian rhythm disturbances. Medications such as benzodiazepines, selective serotonin reuptake inhibitors (SSRIs), and novel agents like dual orexin receptor antagonists and melatonin receptor agonists have been studied for their effects on sleep architecture, specifically focusing on enhancing TST, SWS, and REM sleep.5,6 Despite the widespread use of pharmacological interventions, there is a need to clarify the extent of evidence supporting these medications’ ability to selectively enhance different stages of sleep, particularly SWS and REM sleep, which are crucial for the restorative functions of sleep and to enhance the functions of the glymphatic system.7
While this review focuses primarily on pharmacologic interventions that enhance slow wave sleep, related outcomes including total sleep time and REM sleep are also examined to contextualize medication effects on overall sleep architecture. By mapping the range of pharmacotherapies studied and their effects on these sleep stages, the review aims to identify potential therapeutic strategies, highlight gaps in the literature, and inform future research efforts aimed at optimizing pharmacotherapy for sleep enhancement.
Methodology
This article presents a scoping review of the evidence supporting the effects of various medications on TST, SWS, and REM sleep. The primary focus of this review is the pharmacological modulation of SWS, given its central role in restorative sleep processes and the growing interest in enhancing deep sleep. However, because medications that affect SWS frequently influence other components of sleep architecture, TST and REM sleep were also evaluated to provide a more comprehensive understanding of pharmacologic effects on sleep structure. SWS, also known as delta sleep or N3 sleep of non-rapid eye movement (NREM) sleep, is critical for physical and cognitive restoration, yet remains an underexplored area in pharmacotherapy.1,8
The methodology for this scoping review was based on the protocol outlined by Arksey and O’Malley.9 Since no patient data was used, ethics or Institutional Review Board approval was not obtained for this review.
The following questions guided the literature search, scope, and reporting of findings:
-
What pharmacological treatments have been studied for their effects on SWS?
-
What effects do these medications have on SWS and related aspects of sleep architecture, including TST and REM sleep?
-
What is the mechanism of action by which these medications exert their effects?
-
What gaps remain in the literature, and what directions should future research take?
Search Strategy
Our team of librarians conducted the initial literature search in the Ovid MEDLINE database using the following search terms: delta sleep, stage 3 sleep, stage 4 sleep, REM, rapid eye movement, treatment effect, medications, and pharmacologic.
The literature review was designated to start on January 1st, 1990, after a preliminary search on PubMed revealed an increase in SWS publications under the Results by Year filter. Because this review primarily focuses on pharmacologic interventions affecting SWS, this timeframe was selected to capture the period during which modern polysomnographic studies investigating deep sleep became more common. Studies reporting related sleep architecture outcomes, including total sleep time and REM sleep, were also included when available to provide a more comprehensive assessment of medication effects on sleep. The systematic search was conducted on the publications in the electronic database from January 1st, 1990, to July 30th, 2024. As of July 30th, 2024, unpublished ongoing studies and gray literature, such as conferences, newsletters, and book chapters, were excluded.
All citations (324) were imported into EndNote X8.0.1 (Thomson Reuters). The citations were then deduplicated and uploaded into Covidence (Covidence, Melbourne, Australia), an online tool to help organize and facilitate the literature selection process.
Study Selection
Two team members independently reviewed each title and abstract for the initial screening process. A third member assisted with providing consensus for cases of disagreement. The screening process was iterative. Only articles that discussed the effects of medication on SWS were included. Studies that did not discuss therapeutics were not included. Full articles were obtained, and their references were screened for additional relevant articles.
Charting the Data
The data from primary research articles (studies that generate new data) were compiled in a single spreadsheet. Secondary research articles, such as reviews, were not directly included in the data collection process, but they were consulted to determine additional studies that may not have been included through our screening process.
Results
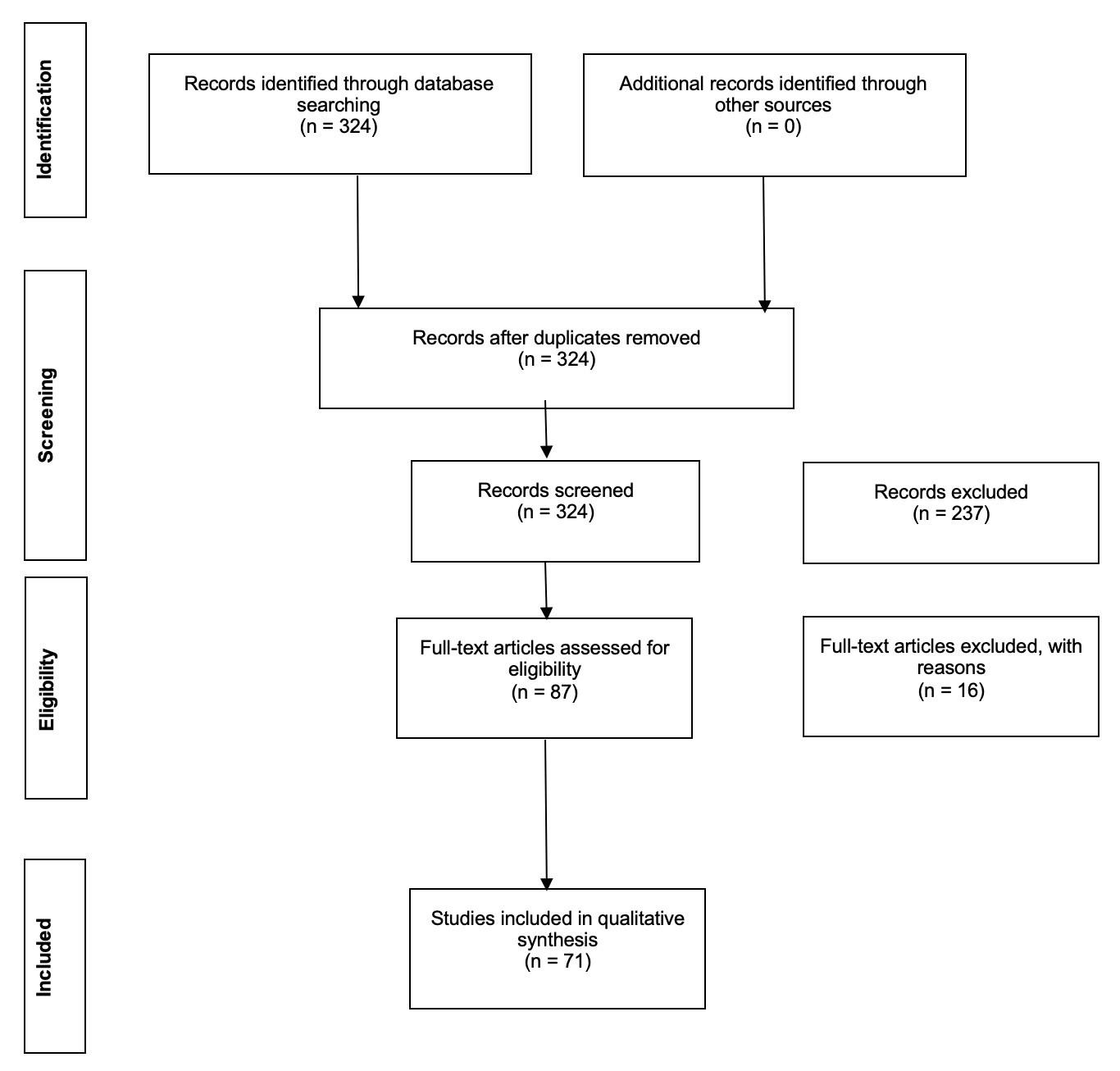
This scoping review identified 324 articles initially screened for relevance. Of these, 253 were excluded because they did not specifically examine the effects of medications on SWS, deep sleep, or REM sleep. Many excluded studies addressed broader topics, such as sleep changes in patients with psychiatric disorders or physiological neurotransmitter fluctuations across sleep stages. 87 articles were eligible for full-text review. 16 articles were excluded because they discussed the pre-translational stage of medication development, such as synthesis and cell culture models. Consequently, a total of 71 articles were included for full-text review. The article screening process is summarized in the PRISMA diagram (Figure 1).
_flow_detailing.jpg)
The 71 articles collectively described 82 unique clinical situations. These studies often examined multiple medications and their effects on SWS, REM sleep, and deep sleep. Notably, individual medications were frequently assessed in diverse patient populations, including:
-
Healthy adults: To establish baseline medication effects on sleep architecture.
-
Patients with insomnia: To explore therapeutic impacts on sleep disruptions.
-
Patients with schizophrenia: To evaluate both psychiatric symptom relief and sleep benefits.
The inclusion of varying populations reflects the broad interest in understanding how medications impact sleep under different physiological and pathological conditions.
Table 1 summarizes medications studied for their effects on TST, SWS, and REM sleep in various patient populations. Given the absence of direct comparative studies, we have employed an arbitrary rating system based on available literature to assess their impact. This system utilizes up and down arrows to represent the degree of change in sleep parameters.
-
One arrow (↑ or ↓) signifies a 0–30% change or a 0–20-minute difference in total time.
-
Two arrows (↑↑ or ↓↓) indicate a 30–60% change or a 20–40-minute difference in total time.
-
Three arrows (↑↑↑ or ↓↓↓) denote a 60–100% change or a 40–60-minute difference in total time.
-
A dash (“-”) represents a non-significant or unchanged effect on total time.
-
An “X” is used when the specific effect was not quantified in the study.
-
Combinations of these symbols, such as ↑/-, indicate that different studies have reported varying effects. Some showed an increase in sleep, while others found no significant change.
Because the primary focus of this review is pharmacologic modulation of SWS, the narrative synthesis below emphasizes SWS-related findings, while TST and REM sleep outcomes are presented in Table 1 to provide additional context regarding broader changes in sleep architecture.
The findings delineate four primary categories of medications that influence TST, SWS, and REM sleep: antipsychotics, neurotransmitter modulators, hormone-based treatments, and dopaminergic agents.
Notably, only three agents produced a 60-100% increase in SWS. This was carbamazepine in healthy adults, parampenel in healthy adults, and GHB in adults with insomnia.17,30
This evaluation system provides a qualitative representation of the available evidence, enabling a structured comparison of medication effects on various aspects of sleep architecture, despite the lack of standardized direct comparisons.
Some medications showed consistent trends in their impact on SWS, while others presented conflicting results across studies. Several drugs, such as antipsychotics, gabapentin, and selective serotonin reuptake inhibitors (SSRIs), were studied extensively but yielded inconsistent findings. For example: One manuscript reported increases in SWS in patients with schizophrenia taking clozapine, while another suggested a decrease in SWS.18,19 These discrepancies highlight the challenge of drawing definitive conclusions about the effects of certain medications.
In addition to inter-study variability, some medications displayed dose-dependent effects on sleep. For instance, apomorphine increased SWS at lower doses but decreased at higher doses, illustrating the nuanced relationship between dosage and sleep architecture.14
Discussion
This review highlights the effects of various pharmacological agents on TST, SWS, and REM sleep, emphasizing their therapeutic potential and the need for further investigation. These agents have diverse mechanisms of action and present a nuanced landscape for clinicians aiming to improve sleep architecture, particularly in patients with psychiatric and neurological conditions.
Effects of Antipsychotic Medications
First- and second-generation antipsychotics were consistently found to enhance both TST and SWS time. Within the second-generation class, medications such as olanzapine, paliperidone, and ziprasidone stood out. These drugs antagonize 5-Hydroxytryptamine receptor 2A (5-HT2A), Dopamine receptor D2 (D2), and alpha-1 adrenergic receptors. This multifaceted receptor activity modulates the dysregulated dopamine and serotonin systems characteristic of schizophrenia.19,43 Importantly, schizophrenia itself is associated with significant disruptions in sleep architecture, including reduced TST and SWS. Thus, some of the sleep benefits observed with these antipsychotic treatments may result not only from the pharmacologic properties of the medications but also from the alleviation of core psychiatric symptoms that contribute to poor sleep.19 These findings suggest that antipsychotics may play a dual role in addressing core psychiatric symptoms while concurrently improving sleep architecture. Interestingly, olanzapine and ziprasidone enhanced SWS sleep in both healthy individuals and individuals with schizophrenia, highlighting the broad applicability of these agents. Among the antipsychotics studied, olanzapine demonstrated the greatest increase in SWS in adults with schizophrenia, with one study demonstrating a 0-30% increase and another reporting a 30-60% increase.19 Nevertheless, the absence of direct comparative studies limits clinicians’ ability to determine the most effective antipsychotic for targeting sleep disturbances.19,43
Neurotransmitter Modulators
Medications targeting the balance between excitatory and inhibitory neurotransmission, such as gamma-hydroxybutyrate (GHB), pregabalin, gabapentin, ketamine, and sodium oxybate, represent a diverse category. These agents primarily enhance SWS and often increase TST.17,30,33,34,43 Among the agents reviewed, GHB produced the greatest increases in SWS for adults with insomnia, with one study demonstrating a 60-100% increase in SWS duration.30 Gabapentin and pregabalin, in particular, are frequently used off-label to improve sleep quality. This is done by binding to the α2δ subunit of voltage-gated calcium channels, thereby reducing excitatory glutamate transmission.43 However, there is limited guidance on whether pregabalin should be initiated only after gabapentin proves to be ineffective, creating a knowledge gap for clinicians.
Hormonal Agents
Hormonal pathways also play an important role in the regulation of sleep architecture. Growth hormone–releasing hormone (GHRH) has been associated with increased SWS, with studies in healthy adults demonstrating a linear relationship between the amount of SWS and growth hormone secretion.31 Melanin-concentrating hormone (MCH), a hypothalamic neuropeptide involved in sleep regulation, has been investigated in rat models for its effects on sleep architecture, though it is not currently an approved therapeutic agent for use in humans.36 Both GHRH and MCH have been shown to increase SWS in experimental studies.31,36 These findings suggest that hormonal pathways influencing sleep may hold promise for future interventions, particularly in populations with disrupted endocrine rhythms.
Dopaminergic Agents and Dose-Response Effects
Dopaminergic D2 receptor agonists (e.g., apomorphine, bromocriptine, quinpirole) emerged as the only investigated class with a dose-response relationship concerning sleep. This finding is significant as it underscores the importance of prescribing proper dosages to minimize adverse effects on sleep architecture. However, the contexts in which these agents are most beneficial for sleep modulation remain poorly understood. Among these D2 receptor agonists, apomorphine was the only agent with a demonstrated increase in 0-30% increase in SWS time at lower concentrations.14 All other investigated dopamine agonists (bromocriptine, pramipexole, ropinirole) demonstrated no significant change except for quinpirole, with a 0-30% decrease in SWS duration.14,42
Differential Effects on REM Sleep
Certain medications enhanced SWS while minimally impacting REM sleep. GABA receptor agonists, such as gaboxadol, tiagabine, THIP, and serotonin antagonists, including agomelatine and trazodone, fell into this category. These agents either maintained or increased TST, making them attractive options for patients with isolated deficits in SWS.11,17,23,27,28 Other GABA agonists, such as 1,4-butanediol, baclofen, GHB, magnesium, and progesterone, increased SWS and REM sleep.10,12,30,34,44 In contrast, medications such as cortisol and 5-HT2A antagonists (e.g., risperidone, olanzapine, and ziprasidone) enhanced SWS while suppressing REM sleep in healthy individuals.19,20,43,46 These findings highlight the diverse effects of sleep-modulating medications and can help providers tailor treatment to specific sleep architecture needs.
Key Knowledge Gaps and Future Directions
This review underscores a lack of comparative effectiveness studies among these diverse agents. For example, clinicians currently have no robust evidence to guide the choice between gabapentin and pregabalin or to determine the best sequence of therapies.17 Similarly, while antipsychotics have been extensively trialed in healthy and schizophrenic populations, their effects on sleep in other psychiatric illnesses remain unexplored.19,43 Further research is urgently needed to:
-
Conduct head-to-head trials comparing the efficacy of medications within and across categories.
-
Investigate the long-term safety and efficacy of these agents in enhancing SWS and REM sleep.
-
Explore their effects in broader patient populations, including those with comorbid psychiatric and sleep disorders.
-
Investigate the dose-dependent effects of medications on SWS and REM sleep.
Conclusion
This review summarizes the mechanisms and effects of various sleep-modulating agents on sleep architecture. However, the lack of comparative data leaves significant gaps in clinical guidance, particularly regarding prioritizing therapies. Until more robust evidence emerges, clinicians must rely on empirical experience and patient-specific factors to guide treatment decisions.
In conclusion, the pharmacological enhancement of SWS and REM sleep remains an evolving field. Promising therapeutic options exist, but substantial knowledge gaps exist. Addressing these gaps through rigorous research is crucial for optimizing sleep interventions and enhancing overall patient outcomes.